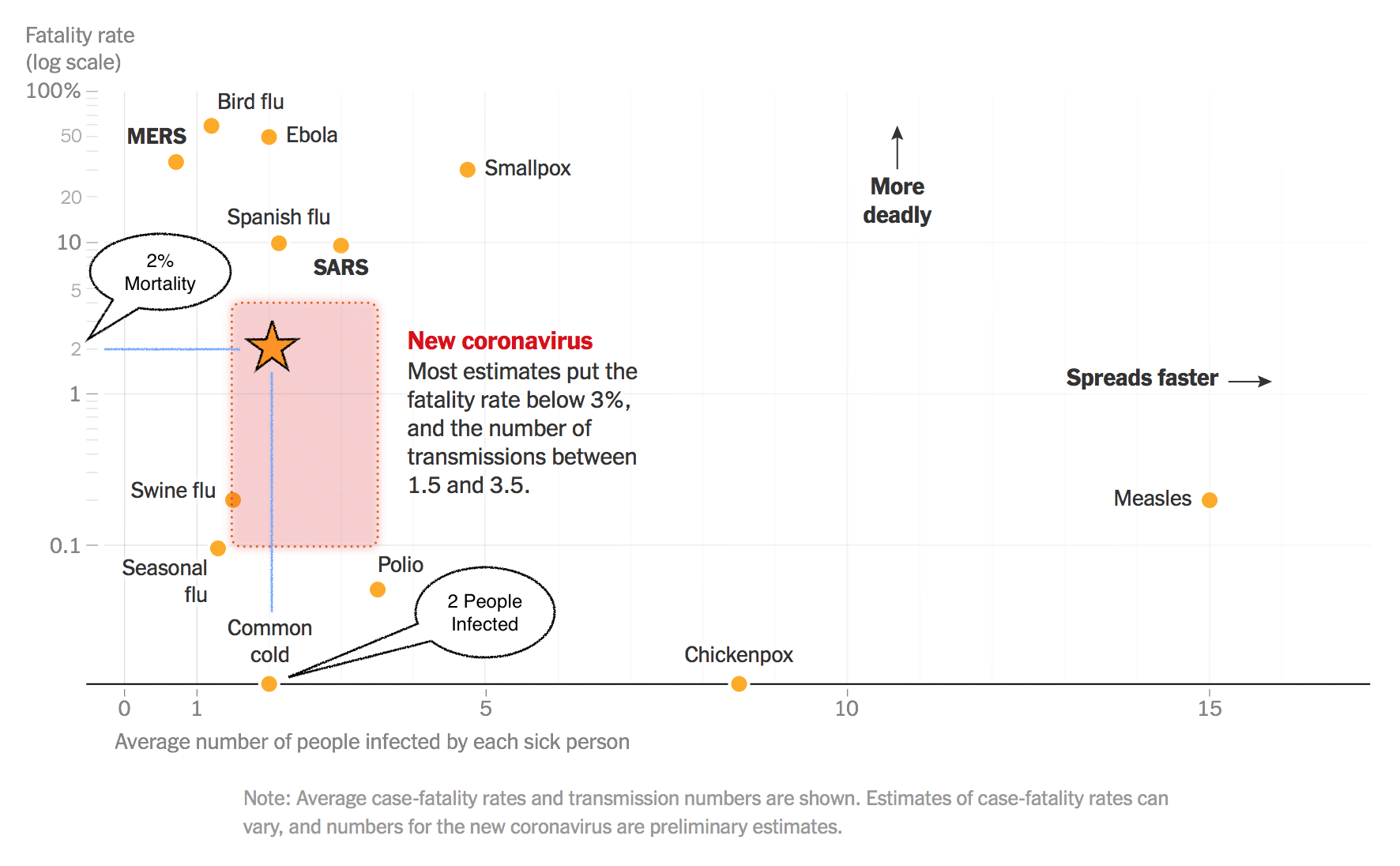
source:nytimes.com (click to enlarge)
I’ve annotated this NY Times graphic, rounding the estimates for COVID19 (aka the 2019 novel coronavirus) to 2% mortality and 2 people infected for every one who has the disease. What this suggests is the infection rate will be similar to a bad cold season, but unlike the common cold, a significant number of people will die of the disease.
This is not good news, but it is also not catastrophic.
By comparison the 1918 “Spanish” Flu had a similar infection rate but killed 1 in 10! The 1918 Flu infected approximately one third of ALL the people on earth… and that was before air travel!
Based on these numbers alone, up to 110 million people in the US could be infected. 80% of these cases should be mild, 20% will need some form of special care in hospitals or at home, and 2% (2.2 million) could die.
One area where the 1918 Flu differs from COVID19 is the latter does not seem to kill children, which is a small bright spot. However, children may be a source of infection for vulnerable adults!
Note that the currently reported mortality rate is over 3% but here in the US we have done almost NO testing, so the total number of infected individuals is unknown, but likely to be much higher. This means the reported mortality rate is probably inflated due to lack of good data. I’ll stick with 2% as a conservative figure for now.
It is also important to remember one of the lessons of the 1918 epidemic, things may look better when warmer weather returns but this should not be reassuring. In the spring of 1918 it looked like the disease was weakening, but it returned with a vengeance in the fall and winter!
Social Isolation and Hand Washing
For the general public, not living with or caring for a sick person, wearing masks really doesn’t help. Social isolation (eg, staying home) and effective hand washing remain the best things you can do to prevent getting most viral respiratory diseases (the common cold, influenza, and the new coronavirus). Just being in the same room with a sick person is not that risky, but touching surfaces and objects in that room and then touching your face is a good way to catch one of these viruses. Note that hand washing studies suggest we generally neglect our fingertips (including the nails) and wrists.
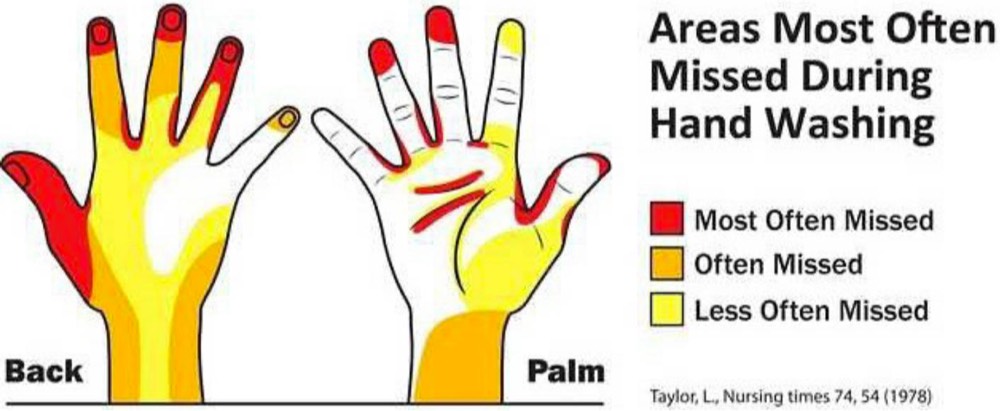
Wash Your Finger Tips!
The best information available comes from CDC and WHO (which I consider the best source since it is not caught up in US political shenanigans). For up-to-date worldwide information download the most recent WHO Situation Report.



 The US Supreme Court is about to hear arguments for and against the recent healthcare insurance reform law enacted by Congress. (aka The Affordable Care Act, aka Obamacare) At issue is the constitutionality of the individual mandate to buy health insurance. It is unclear whether they will set new precedent or rule on a much narrower basis. Their decision could have profound effects on the current law and future legislation. Partisans on both sides of this issue should welcome a broad decision and be ready to accept the consequences!
The US Supreme Court is about to hear arguments for and against the recent healthcare insurance reform law enacted by Congress. (aka The Affordable Care Act, aka Obamacare) At issue is the constitutionality of the individual mandate to buy health insurance. It is unclear whether they will set new precedent or rule on a much narrower basis. Their decision could have profound effects on the current law and future legislation. Partisans on both sides of this issue should welcome a broad decision and be ready to accept the consequences!

